If you have prostate cancer and your doctor has referred you for a PET CT scan — this page explains why it is almost certainly a PSMA PET CT (not a regular FDG scan), what PSMA PET CT shows, when it is used in the prostate cancer journey, what it costs in Delhi, and the one booking instruction that prevents the most common error.
PSMA PET CT for prostate cancer costs ₹14,000–₹20,000 at AERB-licensed nuclear medicine centres in Delhi — compared to ₹28,000–₹42,000 at private hospital radiology departments for the same scan.
The Most Important Thing First — FDG PET CT Does NOT Work for Prostate Cancer
This is the section that prevents the most consequential booking error in the entire PET CT cluster.
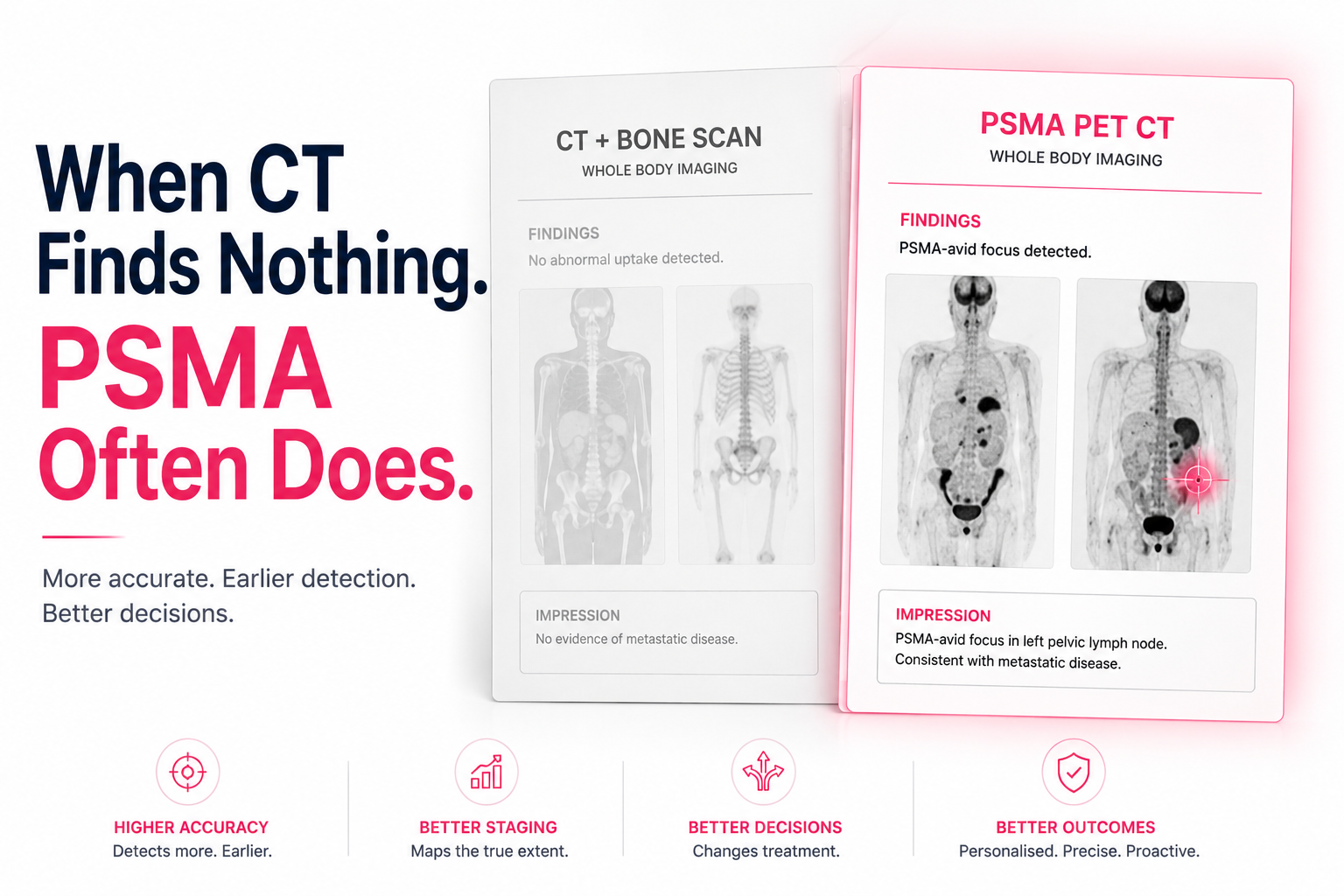
PSMA PET CT has emerged as a highly sensitive imaging modality for prostate cancer, outperforming conventional methods like CT, MRI, and bone scintigraphy.
PSMA PET CT had a 27% absolute greater accuracy compared to conventional imaging — 92% versus 65% — with conventional imaging having lower sensitivity of 38% versus 85% and lower specificity of 91% versus 98%.
Why FDG fails for prostate cancer: Prostate cancer has low glucose metabolism — it is not FDG-avid in the way that lymphoma, lung cancer, and most other solid tumours are. FDG PET CT for prostate cancer frequently produces a scan that shows nothing — not because there is no cancer, but because the cancer does not take up FDG.
What PSMA PET CT uses instead: PSMA (Prostate-Specific Membrane Antigen) is a protein expressed thousands of times more abundantly on prostate cancer cells than on normal cells. Ga-68 PSMA (gallium-68 labelled PSMA tracer) binds specifically to this protein — making even very small prostate cancer deposits visible at PSA levels where CT and bone scan show nothing.
The booking rule: If your prescription says "PET CT for prostate cancer" — it means PSMA PET CT. Not FDG. Confirm "PSMA PET CT" when booking. If your prescription says "PSMA PET CT" explicitly — confirm "Ga-68 PSMA" at the nuclear medicine centre.
Why Prostate Cancer Needs PSMA PET CT — The Clinical Revolution
Prostate cancer staging and recurrence detection changed fundamentally when PSMA PET CT became available. The previous standard — CT scan plus whole body bone scan — missed most prostate cancer metastases at the PSA levels where treatment decisions are most consequential.
The NCCN panel does not feel that conventional imaging is a necessary prerequisite to PSMA PET CT and that PSMA PET CT can serve as an equally effective, if not more effective, front-line imaging tool for patients with prostate cancer.
PSMA PET detected occult disease in 59 to 66% of patients with negative conventional imaging findings in the phase III CONDOR multicenter study of patients with biochemical recurrence. ScienceDirect
What this means in plain language: In 6 out of 10 prostate cancer patients whose CT and bone scan showed nothing — PSMA PET CT found disease. Disease that changes treatment. Disease that the previous standard of care completely missed.
The Four Clinical Scenarios Where PSMA PET CT Is Used
Scenario 1 — Initial Staging: Newly Diagnosed High-Risk Prostate Cancer
PSMA PET CT is indicated for initial risk stratification for localised prostate cancer for patients at unfavourable intermediate, high, or very high risk.
Before surgery (radical prostatectomy) or radiotherapy — PSMA PET CT maps the full extent of disease: is it confined to the prostate, has it spread to pelvic lymph nodes, or are there distant metastases?
Who needs PSMA PET CT at initial staging:
- Gleason score 7b (4+3) or higher
- PSA above 10–20 ng/mL at diagnosis
- Clinical T3 or T4 disease on examination or mpMRI
- Any patient being considered for curative treatment where the presence of distant metastases would change the treatment plan
What it changes: If PSMA PET CT shows pelvic lymph node involvement or distant metastases, the treatment changes from curative-intent surgery or radiotherapy to systemic therapy. This avoids a major surgical procedure that cannot cure disease that has already spread.
Scenario 2 — Biochemical Recurrence: Rising PSA After Treatment
Within 10 years following definitive local therapy for prostate cancer, up to 20–50% of men will develop biochemical recurrence, defined by a rising PSA. MDPI
This is the most common reason for PSMA PET CT referral in Delhi NCR. The patient had prostatectomy or radiotherapy, achieved undetectable PSA, but now PSA is rising. CT scan and bone scan are negative. The question: where is the cancer?

PSMA PET CT answers this question at very low PSA levels:
|
PSA Level |
CT + Bone Scan Detection |
PSMA PET CT Detection |
|
Less than 0.5 ng/mL |
Very low — most patients negative |
36–50% detection rate |
|
0.5 – 1.0 ng/mL |
Low |
57–66% detection rate |
|
1.0 – 2.0 ng/mL |
Low-moderate |
66–75% detection rate |
|
Above 2.0 ng/mL |
Moderate |
80–95% detection rate |
The clinical significance: A rising PSA of 0.3 ng/mL where CT and bone scan are negative does not mean there is no cancer — it means conventional imaging cannot find it. PSMA PET CT detects it in a significant proportion of these patients, enabling targeted salvage treatment (stereotactic radiotherapy to the site of recurrence) rather than systemic hormonal therapy.
Nearly two-thirds of patients in the CONDOR trial experienced a change in their intended management based on PSMA PET CT results — in patients where conventional imaging was negative.
Scenario 3 — Metastatic Castration-Resistant Prostate Cancer (mCRPC) Staging
In patients with metastatic castration-resistant prostate cancer — prostate cancer that has progressed despite hormonal therapy — PSMA PET CT maps the full disease burden to guide treatment selection, including whether Lutetium-177 PSMA therapy is appropriate.
Clinicians should assess non-metastatic castration-resistant prostate cancer patients for development of metastatic disease using conventional or PSMA targeted PET imaging at intervals of 6 to 12 months. PubMed
Scenario 4 — Before Lu-177 PSMA Therapy (Lutetium PSMA Therapy)
Lu-177 PSMA (Lutetium-177 PSMA radioligand therapy) is a targeted radiation treatment for metastatic prostate cancer that uses PSMA-targeting molecules to deliver radiation directly to prostate cancer cells. Before receiving this therapy, a confirmatory PSMA PET CT is essential — to confirm that the patient's prostate cancer cells actually express PSMA at sufficient levels to respond to treatment.
If PSMA PET CT shows adequate PSMA expression across metastatic sites — Lu-177 PSMA therapy is appropriate. If PSMA expression is insufficient — Lu-177 PSMA will not work effectively, and alternative treatments should be considered.
This is one of the most important uses of PSMA PET CT in Delhi's oncology landscape — as Lu-177 PSMA therapy is increasingly available at select centres in India.
PSMA PET CT vs CT + Bone Scan — The Complete Comparison
|
Feature |
CT + Whole Body Bone Scan |
PSMA PET CT |
|
Sensitivity for recurrence |
38% |
85% |
|
Specificity |
91% |
98% |
|
Overall accuracy |
65% |
92% |
|
Detection at PSA < 0.5 ng/mL |
Very low |
36–50% |
|
Bone metastasis detection |
Moderate — bone scan dependent |
Superior |
|
Lymph node metastasis detection |
Low — size-dependent |
Superior — metabolic activity |
|
Soft tissue metastasis |
Limited |
Good sensitivity |
|
Single scan whole body |
No — two separate investigations |
Yes — one investigation |
|
Time required |
2 days (CT + bone scan separate) |
2–3 hours (single visit) |
PSMA PET CT vs FDG PET CT for Prostate Cancer
|
Feature |
FDG PET CT |
PSMA PET CT |
|
FDG/PSMA avidity of prostate cancer |
Low — most prostate cancers not FDG-avid |
High — PSMA highly expressed on PCa cells |
|
Detection of recurrence |
Poor — frequently negative |
Excellent — 85% sensitivity |
|
Use for prostate cancer |
Not recommended |
Standard of care |
|
Cost in Delhi |
₹9,000 – ₹14,000 |
₹14,000 – ₹20,000 |
The rule: never book FDG PET CT for prostate cancer. The scan will almost certainly be negative — not because there is no disease, but because FDG does not target prostate cancer biology.
Understanding Your PSMA PET CT Report
FDG-Avid vs PSMA-Avid: PSMA PET CT reports will describe lesions as "PSMA-avid" rather than "FDG-avid." A PSMA-avid lesion is one showing elevated PSMA tracer uptake — consistent with prostate cancer involvement.
SUVmax on PSMA PET CT: The SUVmax on a PSMA PET CT reflects PSMA tracer uptake intensity. Higher PSMA uptake generally correlates with higher PSMA expression, which has implications for Lu-177 PSMA therapy eligibility. Different SUV thresholds apply compared to FDG — your nuclear medicine physician and urologist interpret this together.
PSMA-Negative Disease: Not all prostate cancers express high PSMA levels. Low PSMA expression (PSMA-negative or low PSMA-avid disease) may indicate a less hormone-sensitive, more aggressive variant — or a cancer that has undergone neuroendocrine differentiation. A negative PSMA PET CT in a patient with rising PSA does not mean no recurrence — it means PSMA expression may be insufficient for detection by this modality.
PSMA PET CT Cost for Prostate Cancer in Delhi 2026
|
Option |
Cost (₹) |
Waiting Time |
Notes |
|
AERB-licensed standalone nuclear medicine centre |
14,000 – 20,000 |
2–5 days |
Same scanner quality |
|
Private hospital (Rajiv Gandhi Cancer, Max, Fortis) |
28,000 – 42,000 |
3–7 days |
Premium pricing |
|
Government centre (AIIMS, IRCH) |
6,000 – 10,000 |
4–10 weeks |
Long wait — not appropriate for biochemical recurrence with rising PSA |
|
CGHS-empanelled nuclear medicine centre |
Confirm current rate |
Same-week |
For CGHS beneficiaries |
The cumulative cost reality for prostate cancer patients: A patient with biochemical recurrence may require PSMA PET CT:
- At the time of recurrence detection
- After salvage treatment to assess response
- At 6–12 monthly intervals during CRPC monitoring
Total: 3–5 PSMA PET CT scans over the treatment course.
At ₹14,000–₹20,000 per scan at a standalone centre versus ₹28,000–₹42,000 at a hospital: the cumulative savings are ₹42,000–₹1,10,000 over the monitoring course.
Preparation for PSMA PET CT
Significantly simpler than FDG preparation:
No carbohydrate restriction. PSMA does not compete with blood glucose — no low-carbohydrate diet required.
Fasting: 4–6 hours before the injection. Water freely.
Hydration: Drink generously before and after the scan. PSMA tracer is excreted through the kidneys — good hydration flushes background activity and improves pelvic image quality.
Urinate just before the scan. The bladder accumulates PSMA tracer — a full bladder creates artefact in the pelvis, exactly where prostate bed recurrence may be present.
Continue all medications including hormonal therapy (ADT — leuprolide, bicalutamide, enzalutamide, abiraterone). There is no need to pause hormonal therapy before PSMA PET CT.
Duration: 2–2.5 hours total at the centre — shorter and simpler than FDG whole body.
Availability in Delhi NCR — PSMA PET CT
PSMA PET CT requires Ga-68 (Gallium-68) tracer — produced by a germanium-gallium generator or cyclotron available at established nuclear medicine centres. Advance booking of 2–5 days is typically required to ensure tracer supply.
|
Area |
PSMA Availability |
Price Range |
Same-Week |
Metro |
|
South Delhi (Green Park, Safdarjung, Saket) |
Yes |
₹14,000 – ₹20,000 |
Yes |
Yellow / Violet |
|
Central Delhi (Karol Bagh, Rajouri) |
Yes |
₹14,000 – ₹20,000 |
Yes |
Blue / Yellow |
|
North Delhi (Rohini) |
Select |
₹14,000 – ₹19,000 |
3–5 days |
Red Line |
|
Noida (Sector 17, 62) |
Select |
₹14,000 – ₹19,000 |
3–5 days |
Blue Line |
|
Gurgaon (Golf Course, Sector 38) |
Select |
₹14,000 – ₹20,000 |
3–5 days |
Yellow Line |
Clinical Note
From the reviewing nuclear medicine physician: The PSMA PET CT story for prostate cancer is one of the most significant advances in oncology imaging I have witnessed in my career. Before PSMA PET CT was available in India, a patient with rising PSA after prostatectomy — say 0.4 ng/mL — had a CT scan and bone scan that showed nothing. We called it biochemical recurrence with no evidence of disease on imaging. The patient went on empirical whole pelvis radiotherapy or hormonal therapy. Now, with PSMA PET CT, I can find a 3mm pelvic lymph node deposit in 50% of these patients — lesions completely invisible to CT. The oncologist can deliver targeted stereotactic radiotherapy to that single node. The patient may achieve durable remission from a targeted treatment that conventional imaging said was unnecessary. The two instructions I give every prostate cancer patient referred for PSMA PET CT in Delhi: first, confirm with your booking team that it is Ga-68 PSMA — not FDG. Second, drink a full 500ml of water before arriving and urinate immediately before entering the scan room. The bladder artefact from PSMA tracer excretion is the single most avoidable technical reason for a suboptimal scan in the pelvic region — and it is entirely in the patient's control.
Book Your PSMA PET CT Scan in Delhi
EVE Healthcare partner centres offer Ga-68 PSMA PET CT scans at AERB-licensed nuclear medicine centres across Delhi, Noida, and Gurgaon — with 2–5 day advance booking for tracer confirmation, same-week availability in most cases, and digital report delivery.
When booking: tell our team "PSMA PET CT for prostate cancer — Ga-68 PSMA." Share your oncologist's referral. Our team confirms tracer availability at the nearest appropriate centre before your appointment is confirmed.
WhatsApp +91 9990032078 or use the search tool at eve-healthcare.com.
Also see: PSMA PET CT Scan Cost Delhi → · FDG vs PSMA vs DOTANOC → · How to Prepare for PET CT → · PET CT Scan Cost Gurgaon → · PET CT Scan Cost Noida → · CGHS PET CT Rate Delhi →