If you have been diagnosed with breast cancer and your oncologist has referred you for a PET CT scan — this page explains when FDG PET CT is used in breast cancer, why the result depends significantly on your specific breast cancer subtype, what it shows at each stage of your treatment journey, and what it costs in Delhi.
FDG PET CT for breast cancer costs ₹9,000–₹14,000 at AERB-licensed nuclear medicine centres in Delhi NCR — the same diagnostic quality as hospital departments at 50–65% lower cost.
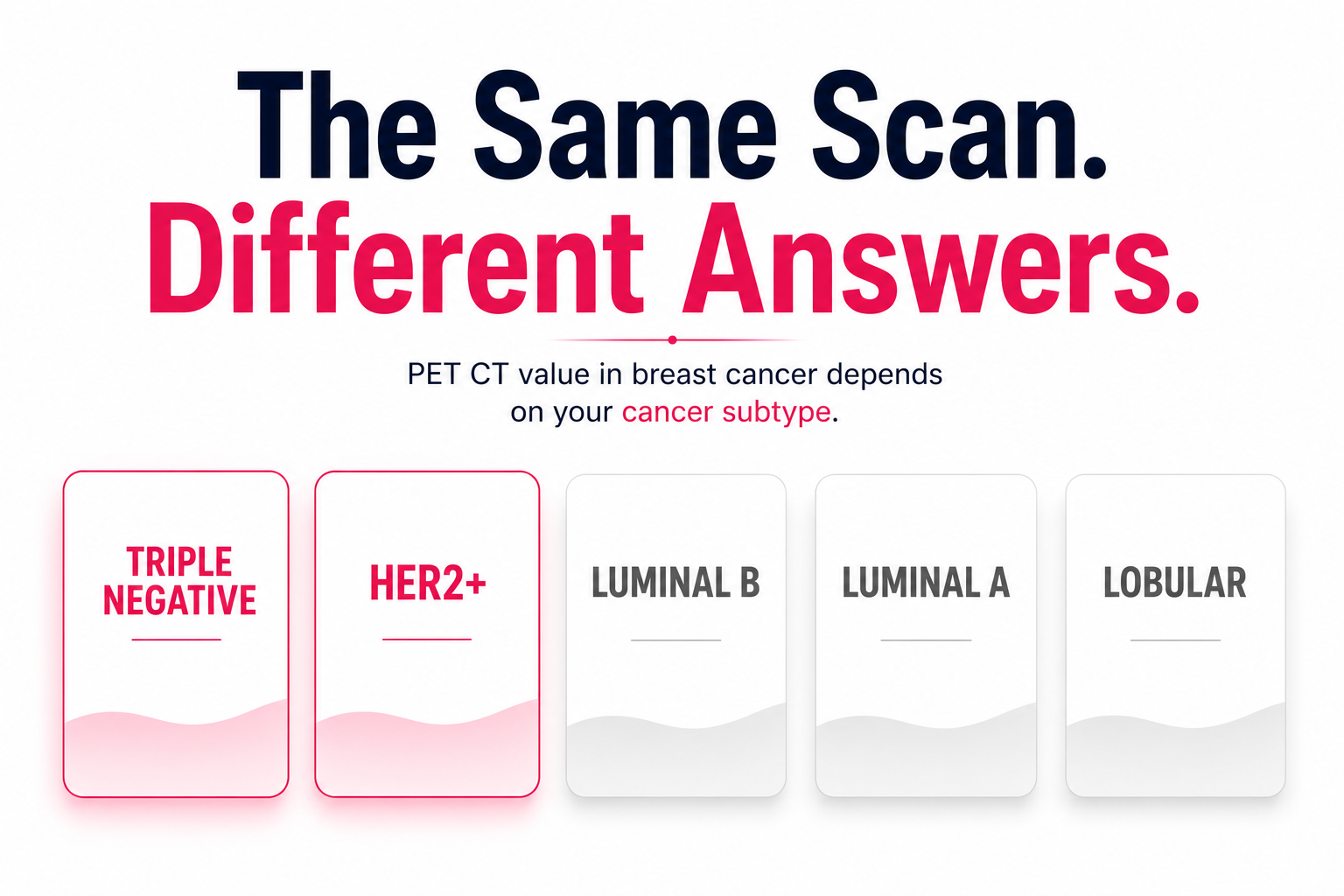
The Most Important Thing to Know First — Your Breast Cancer Subtype Determines How Useful PET CT Will Be
This is the section no competitor page on breast cancer PET CT in Delhi has written. It is the clinical distinction that determines whether your PET CT will be highly informative or potentially misleading.
Luminal type breast cancer tumours have the lowest baseline FDG uptake whilst HER2-positive and triple negative breast cancers have the highest FDG uptake.
What this means for your PET CT:
|
Breast Cancer Subtype |
FDG Avidity |
PET CT Reliability |
|
Triple Negative (ER-/PR-/HER2-) |
High |
Excellent — well detected |
|
HER2-Positive (HER2+) |
Moderate to high |
Good — well detected |
|
Luminal B (ER+, high grade, Ki-67 high) |
Moderate |
Variable — discuss with oncologist |
|
Luminal A (ER+/PR+, low grade, Ki-67 low) |
Low |
Limited — may miss disease |
|
Invasive Lobular Carcinoma |
Low |
Limited — lobular subtype classically FDG-negative |
The practical instruction: Ask your oncologist or breast surgeon — "What is my breast cancer subtype (ER, PR, HER2 status, histological grade, lobular or ductal)?" If you have low-grade luminal A or lobular breast cancer, discuss with your oncologist whether FDG PET CT will provide reliable staging information for your specific case — or whether contrast-enhanced CT and bone scan may be more appropriate.
For triple-negative and HER2-positive breast cancer — FDG PET CT is highly reliable and the investigation provides maximum clinical value.
When Breast Cancer Needs PET CT — The Three Clinical Scenarios
Scenario 1 — Initial Staging: Locally Advanced Breast Cancer
PET CT modified staging for 26% of Stage I breast cancer patients, 29% of Stage IIA, 46% of Stage IIB, 58% of Stage IIIA, and 100% of Stage IIIB patients — detecting distant metastasis in 29% of patients whose pre-PET CT staging had not identified metastatic disease.
For locally advanced breast cancer (Stage IIB and above) — FDG PET CT is the most accurate single investigation for whole-body staging. It maps:
- Primary tumour metabolic activity
- Ipsilateral axillary lymph node involvement
- Internal mammary lymph nodes — frequently missed by conventional imaging
- Supraclavicular lymph nodes
- Contralateral breast and axilla
- Distant metastases — bone, liver, lungs, distant lymph nodes
When PET CT is recommended for initial staging:
- Stage IIB and above (tumour above 5cm, or fixed axillary lymph nodes)
- Any clinical suspicion of distant metastasis — bone pain, breathlessness, elevated liver enzymes
- Inflammatory breast cancer — uniformly recommended
- High-risk early disease where distant staging changes treatment intent
When PET CT is NOT routinely recommended for initial staging:
- Stage I and Stage IIA early breast cancer with low clinical risk — conventional CT and bone scan are used
- Low-grade luminal A histology — where FDG avidity may be insufficient for reliable staging
Scenario 2 — Neoadjuvant Chemotherapy Response Assessment
Neoadjuvant chemotherapy (NAC) — chemotherapy given before surgery — is increasingly used for locally advanced and high-risk breast cancer. FDG PET CT after 2–3 cycles of chemotherapy assesses metabolic response: is the tumour responding to treatment or progressing?
FDG PET CT can monitor metabolic activity in early breast cancer during neoadjuvant systemic therapy. In triple-negative tumours, metabolic breast response predicted pathological complete response with a c-index of 0.82.
The pathological complete response (pCR) question: A pathological complete response — no viable cancer cells in the surgical specimen — is the desired outcome of neoadjuvant chemotherapy. Patients who achieve pCR have significantly better long-term outcomes, particularly in triple-negative and HER2-positive subtypes. FDG PET CT metabolic response after 2–3 cycles is a strong predictor of whether pCR will be achieved.
What a good interim PET CT response looks like: A significant reduction in SUVmax — typically 30% or more from baseline — indicates tumour cells are dying in response to chemotherapy. A complete metabolic response (SUVmax approaching background liver levels, Deauville-equivalent 1–2) predicts pCR with high probability in triple-negative breast cancer.
The treatment adaptation implication: In some protocols — particularly for HER2-positive breast cancer — poor interim PET CT response at cycle 2 may prompt escalation to more intensive regimens or addition of new agents before completing the full course. Your oncologist uses the PET CT response alongside clinical examination and MRI to guide this decision.
Scenario 3 — Suspected Metastatic Recurrence
For breast cancer patients who completed primary treatment (surgery, chemotherapy, radiotherapy) and now have rising tumour markers, bone pain, breathlessness, or abnormal blood tests — FDG PET CT surveys the entire body in a single examination to identify sites of recurrent disease.
The specific sites breast cancer frequently recurs:
- Bone — most common distant site (vertebrae, ribs, pelvis, femur)
- Liver — second most common
- Lungs and pleura
- Brain — particularly in HER2-positive and triple-negative subtypes
- Contralateral axillary or supraclavicular lymph nodes
The bone metastasis detection advantage: FDG PET CT detects metabolically active bone metastases earlier than conventional bone scan — particularly lytic metastases which are FDG-avid but may not show on bone scan until significant bone destruction has occurred.
Brain metastases — the PET CT limitation: The brain has high baseline glucose uptake — brain metastases may be masked on FDG PET CT. If brain metastases are clinically suspected — particularly in HER2-positive or triple-negative patients with neurological symptoms — dedicated MRI brain is required in addition to whole body PET CT.

FDG PET CT vs MRI vs CT for Breast Cancer — What Each Adds
|
Feature |
CT Chest/Abdomen/Pelvis |
Bone Scan |
Breast MRI |
FDG PET CT |
|
Primary tumour extent |
Limited |
N/A |
Superior |
Moderate |
|
Axillary lymph nodes |
Limited |
N/A |
Good |
Good |
|
Internal mammary nodes |
Poor |
N/A |
Variable |
Better |
|
Bone metastases (lytic) |
Poor — misses early |
Variable |
N/A |
Superior |
|
Bone metastases (blastic) |
Good |
Good |
N/A |
Variable |
|
Liver metastases |
Good |
N/A |
N/A |
Good |
|
Lung metastases |
Good |
N/A |
N/A |
Good — but CT better for small |
|
Treatment response |
Size only |
Limited |
Good |
Metabolic change earlier |
|
Whole body in one scan |
Partial |
Whole body |
Body only |
Whole body |
The clinical summary: FDG PET CT's greatest advantage for breast cancer is detecting metabolically active disease across multiple body regions in a single scan — particularly bone metastases that are FDG-avid before they become structurally visible on CT. It does not replace breast MRI for primary tumour assessment, but for whole-body staging and response assessment in FDG-avid subtypes — it is the most comprehensive single investigation.
Delhi-Specific Context — Why Breast Cancer PET CT Matters Here
Breast cancer is the most common cancer in urban Indian women — and Delhi NCR's metropolitan population has among the highest breast cancer incidence rates in India, driven by later age at first childbirth, lower breastfeeding rates, and lifestyle factors associated with urban populations.
The most common presentation in Delhi's oncology centres: locally advanced Stage IIB–III breast cancer — where PET CT staging changes management in approximately 46–58% of patients at these stages. This is the patient group where PET CT provides maximum clinical value.
The most common oncology centres that refer breast cancer patients for PET CT in Delhi NCR: Sir Ganga Ram Hospital, Rajiv Gandhi Cancer Institute, Max Healthcare oncology units, Fortis Memorial, and the AIIMS oncology department. All of these refer to AERB-licensed standalone nuclear medicine centres for PET CT — not exclusively to their own hospital departments.
Baseline PET CT Before Neoadjuvant Chemotherapy — The Booking Priority
For breast cancer patients being referred for PET CT before starting neoadjuvant chemotherapy — the timing is the most important booking consideration. This scan must happen before the first chemotherapy cycle.
Why timing matters for breast cancer specifically: After the first chemotherapy cycle, the metabolic activity of the primary tumour and lymph nodes changes — even without a complete response. A scan performed after the first cycle is no longer a true baseline and cannot be used for reliable pre-versus-post comparison.
The practical timeline: If your first chemotherapy cycle is scheduled in 2 weeks — book your PET CT in the next 3–5 days. EVE Healthcare partner centres offer same-week FDG PET CT appointments across Delhi NCR.
FDG PET CT Cost for Breast Cancer in Delhi 2026
|
Option |
Cost (₹) |
Waiting Time |
Notes |
|
AERB-licensed standalone nuclear medicine centre |
9,000 – 14,000 |
Same-day to 3 days |
Same scanner quality |
|
Private hospital (Rajiv Gandhi Cancer, Max, Fortis) |
25,000 – 38,000 |
3–7 days |
Premium pricing |
|
Government centre (AIIMS, IRCH) |
3,500 – 6,000 |
4–8 weeks |
Not appropriate when pre-NAC baseline is time-sensitive |
|
CGHS-empanelled nuclear medicine centre |
21,000 (CGHS rate) |
Same-week |
CGHS beneficiaries only |
The neoadjuvant chemotherapy cost context: A breast cancer patient receiving neoadjuvant chemotherapy typically requires:
- 1 baseline PET CT (before chemotherapy)
- 1 interim PET CT (after 2–3 cycles in some protocols)
- 1 end-of-treatment PET CT or surgery restaging
Total: 2–3 PET CT scans. At ₹9,000–₹14,000 per scan versus ₹25,000–₹38,000 per scan at a hospital — the cumulative saving is ₹32,000–₹72,000 for identical clinical quality.
Preparation for Breast Cancer PET CT
Standard FDG whole body preparation:
24 hours before: Low-carbohydrate diet — no roti, rice, dal, fruit, or sugar. High-protein meals: chicken, fish, eggs, paneer, green vegetables, plain dahi.
6 hours before: Complete fast — water only. No chai, coffee, juice, or coconut water.
Day of scan: Water freely. Take all regular medications. No exercise.
Breast cancer-specific notes:
Hormonal therapy (tamoxifen, aromatase inhibitors): Continue as prescribed. No pause required before FDG PET CT.
Trastuzumab / pertuzumab (HER2-targeted therapy): Continue as prescribed. Targeted therapy agents do not affect FDG preparation.
Chemotherapy timing for interim PET CT: Performed typically 2–3 weeks after the last chemotherapy cycle — to allow treatment-related inflammatory FDG uptake to settle before the metabolic response can be accurately assessed. Your oncologist specifies the exact timing.
Implants: If you have silicone breast implants — inform the nuclear medicine physician and the centre when booking. This does not contraindicate PET CT but the physician documents it for contextual interpretation.
Full preparation guide → How to Prepare for PET CT →
CGHS for Breast Cancer PET CT
CGHS rate for FDG Whole Body PET CT at NABH-accredited empanelled centres: ₹21,000.
For CGHS beneficiaries with breast cancer — a specialist oncologist referral is required alongside the CGHS CMO referral. Confirm CGHS empanelment and nuclear medicine capability at the specific centre before visiting.
See full CGHS PET CT guide → CGHS PET CT Rate Delhi →
Clinical Note
From the reviewing nuclear medicine physician: The breast cancer PET CT question I encounter most often in Delhi is from patients with locally advanced Stage IIIA or IIIB disease who have just been told they need neoadjuvant chemotherapy. The clinical question is almost always the same: is there distant disease we have not yet found? In my experience with the Delhi NCR patient population — the most common unexpected finding on baseline PET CT for locally advanced breast cancer is bone metastasis, followed by internal mammary lymph node involvement that was not visible on CT. Both findings change the treatment plan — bone metastasis may shift the approach from curative neoadjuvant intent to systemic-first therapy; internal mammary node involvement changes the radiation field. The subtype caveat I always emphasise: in patients with low-grade luminal A or lobular histology, a negative PET CT does not give me the same confidence as a negative PET CT in triple-negative or HER2-positive disease. The FDG avidity difference is real — and it means the nuclear medicine report for a luminal A patient should be interpreted with the awareness that metabolically silent disease may still be present. This is a clinical conversation the patient should have with their oncologist before interpreting a negative PET CT as reassuring across all subtypes.
Book Your Breast Cancer PET CT in Delhi
Tell our team when booking: your chemotherapy start date if this is a baseline scan, your breast cancer subtype (ER/PR/HER2 status) if known, and whether this is an initial staging or response assessment scan. We confirm same-week availability and send preparation instructions before your appointment.
WhatsApp +91 9990032078 or use the search tool at eve-healthcare.com.
Also see: Whole Body PET CT Scan Cost Delhi → · FDG vs PSMA vs DOTANOC → · How to Prepare for PET CT → · PET CT Before Chemotherapy → · CGHS PET CT Rate Delhi → · PET CT Scan Cost Gurgaon