Pregnancy in India involves a specific set of ultrasound scans — governed by clinical guidelines, shaped by Indian law, and experienced with a level of emotional intensity that no other diagnostic investigation matches. This guide covers everything: the complete scan schedule from week 6 to week 40, what each scan actually measures, what the PC-PNDT Act means for your appointment, what the anomaly scan can and cannot detect, what to do if a scan finds something unexpected, and how to understand your reports.
It also gives you the honest information that most pregnancy scan guides in India leave out entirely.
Complete Pregnancy Scan Schedule India 2026 — Quick Reference
|
Scan |
Weeks |
Indian Name |
Purpose |
Mandatory? |
|
Viability / Dating Scan |
6–10 weeks |
Early Pregnancy Scan |
Confirm pregnancy, heartbeat, dates |
Recommended |
|
NT + NB Scan |
11–14 weeks |
NT Scan |
Chromosomal screening, Down syndrome risk |
Recommended |
|
Double Marker Blood Test |
11–13 weeks |
Double Marker |
Combined with NT for risk calculation |
Recommended |
|
Level 1 Ultrasound |
16–18 weeks |
Level 1 / Screening USG |
Anatomy overview, placenta, fluid |
Recommended |
|
Level 2 / Anomaly Scan |
18–22 weeks |
TIFFA Scan / Anomaly Scan |
Detailed fetal anatomy — 20+ structures |
Mandatory for all |
|
Fetal Echocardiography |
20–24 weeks |
Fetal Echo |
Detailed fetal heart assessment |
If indicated / high-risk |
|
Growth Scan |
28–32 weeks |
Growth Scan / Fetal Wellbeing |
Growth, amniotic fluid, placental grade |
Recommended |
|
Colour Doppler |
28–32 weeks |
Doppler USG |
Umbilical and fetal blood flow |
If IUGR suspected |
|
Third Trimester Scan |
34–36 weeks |
Late Growth Scan |
Presentation, placenta, growth |
Recommended |
|
Biophysical Profile (BPP) |
As advised |
BPP |
Fetal wellbeing score — 5 parameters |
If indicated |
|
Pre-Delivery Scan |
37–40 weeks |
Presentation Scan / BPP |
Fetal position, fluid, delivery planning |
Recommended |
The Federation of Obstetric and Gynaecological Societies of India (FOGSI) and the Government of India recommend a minimum of three to four scans during a normal pregnancy, with additional scans advised for high-risk pregnancies. CRPF
Pregnancy Ultrasound Cost in Delhi NCR — Complete Price Guide 2026
|
Scan |
Standalone Lab (₹) |
Private Hospital (₹) |
CGHS Rate NABH (₹) |
|
Viability / Dating Scan |
700 – 1,500 |
2,000 – 4,000 |
425 |
|
NT Scan (NT + NB) |
1,500 – 3,500 |
4,000 – 8,000 |
850 |
|
Level 1 Ultrasound |
1,000 – 2,500 |
3,000 – 6,000 |
850 |
|
Level 2 Anomaly Scan (TIFFA) |
2,000 – 5,000 |
5,000 – 12,000 |
1,700 |
|
Fetal Echocardiography |
3,000 – 8,000 |
8,000 – 15,000 |
2,125 |
|
Growth Scan |
800 – 2,500 |
2,500 – 6,000 |
425 |
|
Colour Doppler |
1,500 – 4,500 |
4,000 – 9,000 |
850 |
|
Biophysical Profile (BPP) |
1,500 – 3,500 |
3,500 – 7,000 |
850 |
|
3D / 4D Ultrasound |
2,000 – 6,000 |
5,000 – 12,000 |
Not covered |
|
Pre-Delivery / Presentation Scan |
1,000 – 2,500 |
3,000 – 6,000 |
425 |
All prices from EVE Healthcare partner centres in Delhi NCR — NABL-accredited standalone labs. Hospital rates for comparison only. CGHS rates from official rate schedule effective October 2025. Prices verified June 2026.
EVE Healthcare Insight — Pregnancy Scan Booking Data Delhi NCR 2025–2026
|
Metric |
Data |
|
Most booked scan type |
Anomaly Scan |
|
Average booked price — anomaly scan |
₹ 3000 |
|
Average booked price — NT scan |
₹ 2500 |
|
Most booked area for pregnancy scans |
South Delhi |
|
Most common reason for repeat anomaly scan |
Suboptimal fetal position |
Before Your First Scan — What the PC-PNDT Act Means for Your Appointment
This is the section that every Indian pregnancy scan guide omits entirely. It is the most practically important information for any woman attending her first ultrasound in India.
What the law is:
The core mandate of the PC-PNDT Act is clear: it is illegal to determine or disclose the sex of a fetus before birth using any diagnostic technique — including ultrasound, blood tests like NIPT, amniocentesis, and chorionic villus sampling. Wikipedia
The PC-PNDT Act (Pre-Conception and Pre-Natal Diagnostic Techniques Act) was enacted in 1994 in response to a severe demographic crisis caused by sex-selective abortion. At the time of enactment, an estimated 70% of all abortions performed in Delhi were due to the fetus being female. The law is strictly enforced. A doctor who communicates fetal sex faces imprisonment of up to three years and cancellation of their medical licence. Dr. Abhishek Gandhi
What this means at your appointment — practically:
Every ultrasound centre in India that performs obstetric scans is required to be registered under the PC-PNDT Act. When you arrive for any pregnancy scan, you will be asked to complete Form F — a mandatory government document. Here is what to bring and expect:
|
Requirement |
What to Bring / What to Expect |
|
Form F |
Completed at the centre — staff will give it to you. Requires basic details about the pregnancy and its indication |
|
Photo ID |
Aadhaar card is the most widely accepted. Bring the original |
|
Declaration |
You sign a declaration that you are not requesting the scan for the purpose of sex determination |
|
Doctor's declaration |
The performing doctor signs a declaration that fetal sex was not determined or communicated |
|
Companion restrictions |
Some centres restrict companions during the scan — in some states including Delhi, husbands may not be allowed inside the scan room itself due to PC-PNDT enforcement |
Why the sonographer will not tell you the sex:
This is not a centre policy — it is criminal law. Any medical professional who communicates the fetal sex risks imprisonment, a fine, and cancellation of their medical licence. The sonographer will not hint, gesture, or respond to indirect questions. This applies to every diagnostic technique including NIPT blood tests. Do not ask, and do not be offended when a good doctor firmly declines. Wikipedia
The companion restriction explained:
In some states, husbands and relatives have been banned from ultrasound rooms after instances where companions recorded videos and photographs to determine the fetal sex and shared them on public platforms. Delhi NCR centres vary in their companion policy — some allow one companion in the room, others do not. Confirm when booking rather than assuming your partner will be present throughout. Wikipedia
First Trimester — Months 1 to 3
The Viability Scan (6–10 Weeks)
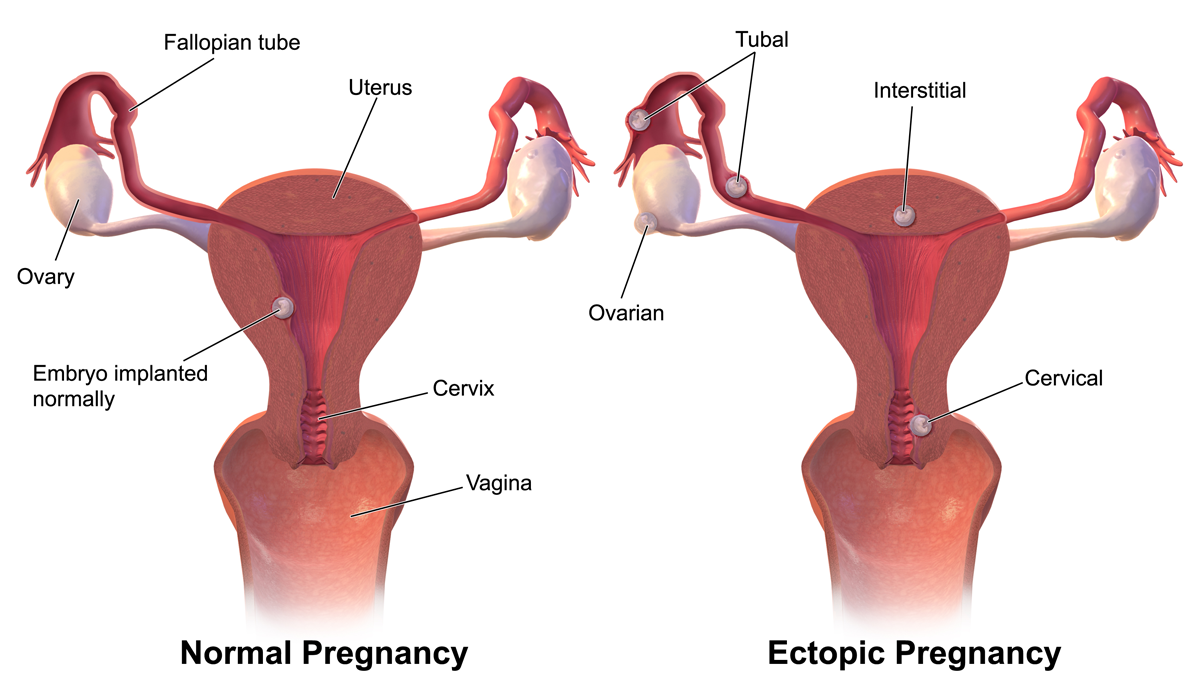
The first scan of pregnancy. It answers four questions: is the pregnancy in the right place (uterine, not ectopic)? Is there a heartbeat? How many babies? And when is the due date?
A heartbeat between 120 and 160 beats per minute at this stage is reassuring. The scan is often done transvaginally in early weeks — a small probe is gently inserted into the vagina for a clearer image. This is entirely safe and not painful, though it may feel mildly uncomfortable. Many women are surprised to find it is the clearest image they will see of their baby in early pregnancy.
What the report should say: Intrauterine pregnancy (not ectopic), fetal pole visible, cardiac activity present, CRL (Crown-Rump Length) measurement for dating, one sac/one fetus (or more).
What it cannot assess: Chromosomal conditions, structural anatomy, placental position. This is not an anomaly screen — it is a viability and dating confirmation.
The NT Scan — 11 Weeks to 13 Weeks 6 Days
The Nuchal Translucency (NT) scan is the most clinically important scan of the first trimester and one of the most anxiously awaited.
What it measures: The NT is the fluid-filled space at the back of the fetal neck. When this space is enlarged, it increases the statistical risk for Down syndrome (Trisomy 21), Edwards syndrome (Trisomy 18), Patau syndrome (Trisomy 13), and certain heart defects. It does not diagnose any of these conditions — it calculates a probability.
The combined first-trimester screen: The NT measurement combined with two blood tests — PAPP-A (pregnancy-associated plasma protein-A) and free beta-hCG — produces a combined risk score. This is far more accurate than the NT measurement alone.
What a high NT means — and what it does not mean:
An elevated NT is not a diagnosis. It is a statistical flag. The majority of fetuses with a high NT measurement are born completely healthy. What a high NT result means in practice is that your obstetrician will recommend further testing — usually either NIPT (a non-invasive blood test) or diagnostic testing (amniocentesis or CVS).
|
NT Result |
What Happens Next |
|
Low risk (combined score less than 1 in 250) |
Routine anomaly scan at 18–22 weeks. No additional testing typically needed |
|
Intermediate risk (1 in 250 to 1 in 1000) |
NIPT offered as next step — high sensitivity, no risk to the pregnancy |
|
High risk (greater than 1 in 250 combined) |
Diagnostic testing discussed — amniocentesis or CVS for definitive chromosomal result |
|
NT above 3.5mm regardless of combined score |
Referral to Fetal Medicine Specialist recommended — higher cardiac and structural anomaly risk |
The Nasal Bone (NB): The NT scan also assesses whether the nasal bone is visible. An absent nasal bone at this stage increases Down syndrome risk. It is not a definitive finding but contributes to the risk calculation.
Timing is critical: The NT scan has a narrow window — 11 weeks 0 days to 13 weeks 6 days. If you miss this window, the NT measurement cannot be taken. Book in advance.
Second Trimester — Months 4 to 6
The Level 2 Anomaly Scan (TIFFA) — 18–22 Weeks
The anomaly scan is the most important scan of pregnancy — and the one that carries the most emotional weight. It is also the scan that most Indian pregnancy guides describe least honestly.
What it checks: The TIFFA (Targeted Imaging for Fetal Anomalies) scan is a detailed structural survey of the fetus. A trained sonographer systematically examines 20+ fetal structures across approximately 45–60 minutes. The checklist includes:
|
System |
What Is Assessed |
|
Brain |
Cerebral ventricles, corpus callosum, cerebellum, cisterna magna |
|
Face |
Lips, palate profile, orbits, nasal bone |
|
Heart |
Four-chamber view, outflow tracts, size and position |
|
Spine |
Vertebral column, skin covering, sacrum |
|
Abdomen |
Stomach, kidneys, bladder, abdominal wall, cord insertion |
|
Limbs |
All four limbs, hands, feet, bone lengths |
|
Placenta |
Location, appearance, relation to cervical os |
|
Amniotic fluid |
AFI measurement |
|
Cervix |
Length — if indicated |
The honest picture on what the anomaly scan detects:
The fetal anomaly scan detection rate for major structural malformations ranges from 15% to exceeding 90% in some cases — with overall detection rates ranging from 46% to 76%. ClinicSpots
In India, additional systemic, infrastructural, and legal factors further restrict anomaly detection effectiveness — particularly for subtle, complex, or late-onset fetal abnormalities. LabsAdvisor
The range is wide because detection depends on multiple factors:
|
Factor |
Impact on Detection |
|
Fetal position on the day of scan |
Baby must cooperate — some structures cannot be seen if fetal position is unfavourable |
|
Sonographer experience and training |
The single biggest variable in detection quality |
|
Machine quality |
High-end machines detect subtle findings that basic machines miss |
|
Specific anomaly type |
Gastroschisis (abdominal wall defect): near 100% detection. Aortic coarctation (heart): as low as 22% |
|
Stage of pregnancy |
Some anomalies develop or become visible later than 22 weeks |
|
Maternal factors |
Obesity, scarring, and fluid levels affect image quality |
What the anomaly scan cannot guarantee:
The ultrasound report typically bears a disclaimer, signed by the patient, acknowledging that some fetal abnormalities might not be detected due to technical limitations. Indian courts have upheld this disclaimer — a missed prenatal diagnosis does not automatically constitute negligence when established protocols are followed. LabsAdvisor
This is not reassuring marketing — it is the clinical reality. The anomaly scan is the best available screening tool. It is not infallible. A completely normal anomaly scan significantly reduces the probability of a major structural anomaly — it does not eliminate it.
Should You Get Your Anomaly Scan at a Fetal Medicine Specialist or a Routine Sonographer?
This is the question no competitor guide answers. It directly affects the quality of your anomaly scan.
A routine sonographer performs the standard 18-point anatomy checklist. Appropriate for most low-risk pregnancies at a well-equipped NABL-accredited standalone diagnostic centre with a trained obstetric sonographer.
A Fetal Medicine Specialist (FMS) is a doctor with additional training in obstetric ultrasound and prenatal diagnosis. They perform more detailed structural assessment, interpret soft markers (choroid plexus cysts, echogenic bowel, short femur), counsel for equivocal findings, and coordinate invasive testing if needed.
When to choose a Fetal Medicine Specialist:
|
Situation |
Choose FMS? |
|
First pregnancy, age under 35, no risk factors, normal NT |
Routine sonographer at NABL lab sufficient |
|
Age 35 or above |
FMS recommended |
|
Previous pregnancy with chromosomal or structural anomaly |
FMS strongly recommended |
|
Abnormal or high-risk NT result |
FMS required |
|
Family history of chromosomal condition or structural heart defect |
FMS strongly recommended |
|
Diabetes, hypertension, or other maternal medical condition |
FMS recommended |
|
Previous unexplained pregnancy loss |
FMS recommended |
|
Twins or multiple pregnancy |
FMS recommended |
Fetal Medicine Specialist centres in Delhi NCR: Sir Ganga Ram Hospital, Artemis Hospital Gurgaon, Fortis Memorial Research Institute Gurgaon, Moolchand Hospital, and dedicated standalone fetal medicine units in South Delhi. Confirm availability and booking process when booking through EVE Healthcare.
What Happens If the Anomaly Scan Finds Something
This is the most-searched, least-answered question in Indian pregnancy ultrasound content. Every guide says "consult your doctor." This page tells you what actually happens.
When an ultrasound examination reveals abnormal findings, it is a shock for the parents-to-be. Women often experience emotional reactions such as anxiety, prostration, depression, and loneliness, as well as guilt, fear, sadness, or hopelessness. This is a documented clinical reality — not an exaggeration. If you receive unexpected news at your anomaly scan, what you feel is both normal and supported by research. Wikipedia
The actual pathway after an anomaly scan finding:
Step 1 — Immediate response: The sonographer completes the scan and records the findings. You will be given a written report. You may or may not be told details at the centre — some sonographers explain findings, others instruct you to return to your obstetrician for discussion. Either is normal.
Step 2 — Obstetrician consultation: Your obstetrician reviews the finding in the context of your complete clinical history — age, family history, NT result, blood tests. The finding is classified as a major structural anomaly, a minor soft marker, an uncertain finding, or a normal variant.
Step 3 — The pathway depends on the finding type:
|
Finding Type |
What Typically Happens Next |
|
Major structural anomaly (e.g. neural tube defect, cardiac defect) |
Immediate referral to Fetal Medicine Specialist. Detailed cardiac echo if heart involved. Genetic counselling. Options discussion |
|
Soft marker (e.g. choroid plexus cyst, echogenic intracardiac focus) |
Risk recalculation with all findings combined. NIPT or amniocentesis discussed if risk elevated |
|
Uncertain finding |
Repeat scan at 24–26 weeks by FMS. Majority of uncertain findings resolve on repeat imaging |
|
Placental or fluid finding |
Additional monitoring scans scheduled. Not necessarily a fetal problem — may indicate monitoring need |
Step 4 — If further testing is recommended:
NIPT (Non-Invasive Prenatal Testing): A maternal blood test that analyses fetal DNA fragments. Sensitivity above 99% for Down syndrome, Edwards, and Patau. No risk to the pregnancy. Results in 7–14 days. Does not diagnose structural anomalies — chromosomal only.
Amniocentesis: A needle guided by ultrasound removes a small amount of amniotic fluid containing fetal cells. Definitive chromosomal diagnosis. Performed at 16 weeks or later. Carries a small risk of miscarriage (approximately 0.5–1% at experienced centres). Results in 2–3 weeks.
CVS (Chorionic Villus Sampling): Placental tissue sampling. Earlier than amniocentesis — can be done from 11 weeks. Definitive chromosomal result. Similar miscarriage risk. Results in 1–2 weeks.
Step 5 — Information, not pressure: The role of fetal medicine, genetic counselling, and your obstetrician at this stage is to provide complete information about the finding, its implications, and your options. No decision is required immediately. In India, termination of a pregnancy with significant fetal anomaly is permitted under the Medical Termination of Pregnancy (MTP) Act — up to 24 weeks, and beyond 24 weeks in specific circumstances with appropriate approvals. This decision, if it arises, is entirely yours to make with complete medical information and counselling support.
Third Trimester — Months 7 to 9
ISUOG's 2024 third-trimester guidelines encompass determination of placental location and fetal presentation, measurement of fetal biometry, identification of fetal anomalies, evaluation of amniotic fluid volume, and documentation of fetal and uterine artery Doppler findings. Medifee
The Growth Scan — 28 to 32 Weeks
The growth scan measures how the baby is growing and checks the environment they are growing in.
What is measured:
|
Measurement |
What It Means |
|
BPD (Biparietal Diameter) |
Width of the fetal skull — estimates gestational age and growth |
|
HC (Head Circumference) |
Total head circumference |
|
AC (Abdominal Circumference) |
The most sensitive indicator of fetal growth — reflects nutritional status |
|
FL (Femur Length) |
Length of the thigh bone |
|
EFW (Estimated Fetal Weight) |
Calculated from the above — plotted against gestational age norms |
|
AFI (Amniotic Fluid Index) |
Total amniotic fluid in four quadrants — normal range 8–18 cm |
|
Placental Grade |
0–3 scale of placental maturity |
Understanding the EFW percentile: The EFW is plotted on a growth chart against what is expected at that gestational age. A baby between the 10th and 90th percentile is considered normally grown. Below the 10th percentile raises the question of IUGR (intrauterine growth restriction), which may require additional Doppler assessment and monitoring.
Decoding Your Third Trimester Report — What the Terms Mean
This section exists nowhere else in the Indian pregnancy scan content space. It is what women photograph and share in pregnancy WhatsApp groups.
|
Report Term |
Normal Range |
What It Means If Abnormal |
|
AFI (Amniotic Fluid Index) |
8 – 18 cm |
Below 5 cm (oligohydramnios): possible kidney issue or placental insufficiency. Above 24 cm (polyhydramnios): possible GDM, fetal swallowing problem |
|
BPP Score |
8/10 or 10/10 |
Score of 6: borderline — repeat in 24 hours. Score 4 or below: immediate obstetric review |
|
Placental Grade |
Grade 0–2 before 36 weeks |
Grade 3 before 36 weeks: may indicate accelerated placental ageing — requires clinical correlation |
|
S/D Ratio (Umbilical Artery Doppler) |
Less than 3.0 after 30 weeks |
Elevated: increased placental resistance — IUGR monitoring |
|
Absent End-Diastolic Flow |
Abnormal finding |
Indicates severe placental compromise — immediate obstetric management |
|
Reversed End-Diastolic Flow |
Abnormal finding |
Indicates critical placental compromise — emergency obstetric assessment |
|
MCA PI (Middle Cerebral Artery) |
Greater than 1.0 |
Brain-sparing: fetus redirecting blood to brain — sign of compromise |
|
Cervical Length |
Greater than 25mm at 24 weeks |
Below 25mm: preterm labour risk — may require intervention |
|
Placenta Previa |
Placenta not covering os |
Complete previa: caesarean delivery planning — no vaginal delivery |
"Grade 3 placenta" before 36 weeks: This is the finding most commonly misunderstood by women reading their own reports. A Grade 3 placenta does not automatically mean something is wrong. It indicates placental calcification consistent with maturation. Before 36 weeks, it warrants clinical attention and possibly a repeat scan. After 36 weeks, it is common and not necessarily clinically significant. Your obstetrician interprets this in the context of your full clinical picture — not in isolation.
Colour Doppler — When Is It Needed?
Colour Doppler is not part of every growth scan — it is ordered when your obstetrician suspects placental insufficiency, growth restriction, or fetal compromise.
What it measures: Blood flow velocity in the umbilical artery (placenta to fetus), the middle cerebral artery (in the fetal brain), and sometimes the ductus venosus (in the fetal liver). These measurements reveal whether the placenta is functioning adequately and whether the fetus is compensating for reduced blood flow.
Cost in Delhi NCR: ₹1,500–₹4,500 at standalone labs. ₹4,000–₹9,000 at private hospitals.
The Biophysical Profile (BPP)
The BPP assesses five parameters of fetal wellbeing in real time, each scored 0 or 2:
|
Parameter |
What Is Observed |
Score |
|
Fetal breathing movements |
At least one episode of 30+ seconds in 30 minutes |
0 or 2 |
|
Fetal movements |
At least 3 body movements in 30 minutes |
0 or 2 |
|
Fetal tone |
At least one extension/flexion of limb or spine |
0 or 2 |
|
Amniotic fluid |
AFI greater than 2cm in one quadrant |
0 or 2 |
|
NST (Non-Stress Test) |
Reactive fetal heart rate pattern |
0 or 2 |
Total score interpretation:
- 8–10: Normal. Low risk of fetal compromise
- 6: Equivocal — repeat within 24 hours
- 4 or below: Abnormal — immediate obstetric review required
CGHS Rates for Pregnancy Scans in Delhi
Central Government employees and pensioners with CGHS cards are entitled to pregnancy scans at official CGHS rates at empanelled centres.
|
Scan |
Non-NABH Rate (₹) |
NABH Rate (₹) |
|
Ultrasound (Obstetric / Dating / Growth) |
360 |
425 |
|
NT Scan |
723 |
850 |
|
Level 2 / Anomaly Scan (TIFFA) |
1,445 |
1,700 |
|
Fetal Echocardiography |
1,808 |
2,125 |
|
Colour Doppler (Obstetric) |
723 |
850 |
|
Biophysical Profile |
723 |
850 |
|
Transvaginal Ultrasound |
360 |
425 |
Source: CGHS Rate Schedule effective October 2025, Ministry of Health & Family Welfare, Government of India.
For CGHS bookings: Bring your CGHS Smart Card, a valid referral letter from your CGHS CMO or empanelled gynaecologist, and Aadhaar card. Confirm CGHS empanelment before visiting. Note that CGHS does not cover 3D/4D ultrasound — this is considered a non-essential elective scan.
Preparation for Each Scan — What Actually Matters
Most guides say "full bladder." This is incomplete and for some scans actively wrong.
|
Scan |
Correct Preparation |
|
Viability scan (transabdominal) |
Full bladder — drink 4–6 glasses of water 1 hour before, do not urinate before the scan |
|
Viability scan (transvaginal) |
Empty bladder — urinate just before the scan |
|
NT Scan |
Full bladder. Do not fast — eat normally |
|
Level 2 Anomaly Scan (TIFFA) |
Full bladder. Eat normally — a light meal 1–2 hours before may help fetal activity |
|
Growth Scan |
No bladder preparation needed beyond normal hydration |
|
Colour Doppler |
No special preparation |
|
Fetal Echo |
No special preparation — baby's heart is always visible |
|
BPP |
No special preparation |
|
Pre-delivery scan |
No special preparation |
The most common preparation mistake EVE patients make: Arriving for a transvaginal viability scan with a full bladder — then being told to urinate and wait another 20 minutes. Confirm with the centre whether the scan will be transabdominal or transvaginal when booking.
What to wear: Loose, comfortable clothing. A two-piece outfit (top and trousers or skirt) is more practical than a dress — the sonographer needs access to the abdomen and sometimes the lower pelvis.
Bring to every scan:
- Previous scan reports and CDs — the sonographer compares previous measurements
- Your Aadhaar card and CGHS card if applicable
- Form F will be provided at the centre — no need to download in advance
3D and 4D Ultrasound — Clinical Use vs Keepsake
Many centres in Delhi NCR offer 3D and 4D ultrasound during pregnancy. Understanding what these are — and what they are not — prevents a misunderstanding that affects many Indian families.
3D ultrasound: A static three-dimensional image of the fetal surface. Shows facial features, limb structure, and external anatomy in detail.
4D ultrasound: A real-time 3D image — essentially a video of the baby in the womb. Shows movements, expressions, and behaviour.
Clinical use: 3D/4D ultrasound has specific clinical applications — fetal lip and palate assessment, evaluation of uterine anomalies, assessment of umbilical cord insertion. In these specific situations, it is clinically meaningful.
Keepsake use: Most 3D/4D scans in India are booked by parents wanting to see their baby's face — entirely understandable. These scans are not medically necessary and are not covered under CGHS. If you choose to have one, ensure it is performed at an NABL-accredited centre by a trained sonographer — not at a commercial "baby photo" studio with untrained operators.
The safety note: Ultrasound is safe. Extended scanning sessions purely for photography purposes — without a clinical indication — are not recommended because of the ultrasound energy exposure time. A focused 10–15 minute 3D scan at a clinical centre is very different from a 45-minute photography session. Choose centres appropriately.
The Emotional Dimension — What Research Says About Pregnancy Scan Anxiety
The overall prevalence of psychological morbidities during pregnancy is 14.6%, with anxiety and depression being the leading ones. Pregnancy scan appointments — particularly the anomaly scan — are among the most anxiety-provoking moments of the pregnancy for most women. Koshikaa
When an ultrasound examination reveals abnormal findings, it is a shock for the parents-to-be. Women often experience emotional reactions such as anxiety, prostration, depression, and loneliness, as well as guilt, fear, sadness, or hopelessness. Women begin grieving at the time of the fetal ultrasound examination itself. Wikipedia
This is not a warning designed to frighten you. It is a recognition that the emotional stakes of pregnancy scans are real — and that the way you approach a scan appointment affects your experience of it.
What helps:
- Knowing what the scan will and will not check before you go in
- Understanding that a normal scan does not guarantee a perfect outcome — and that an abnormal finding does not guarantee a poor one
- Having someone with you in the waiting room even if they cannot be in the scan room
- Asking the sonographer at the start of the scan to explain what they are looking at as they go — many will do this if asked
What to do if you receive unexpected news: Do not try to interpret scan findings alone from Google. Call your obstetrician before searching online — most findings that appear alarming on a report have a nuanced clinical explanation. Ask for a follow-up appointment the same day or the next morning. You are entitled to a full explanation of what was found, what it may mean, and what the next steps are.
Is It Safe to Have Multiple Ultrasound Scans During Pregnancy?
Yes. Obstetric ultrasound uses sound waves — not radiation. It does not use X-rays or ionising radiation of any kind. The safety of ultrasound during pregnancy has been studied for over 50 years. No adverse effects on fetal development have been found from diagnostic ultrasound used appropriately.
The number of scans listed in this guide — 6 to 9 for a normal pregnancy, more for high-risk — is clinically standard in India and internationally. Each scan has a specific clinical purpose. There is no evidence that having this number of scans causes harm.
Book Your Pregnancy Scans in Delhi Through EVE Healthcare
EVE Healthcare partner centres offer the complete range of pregnancy ultrasound scans across Delhi, Noida, and Gurgaon — NABL-accredited machines, experienced obstetric sonographers, CGHS rates at empanelled centres, and digital report delivery.
When booking your anomaly scan through EVE: tell our team your gestational age, any previous NT or blood test results, and whether you are high-risk. We confirm sonographer experience level and whether a Fetal Medicine Specialist is available at that centre.
WhatsApp +91 9990032078 or use the search tool at eve-healthcare.com.
Also see: Ultrasound Cost Delhi → · NT Scan Cost Delhi → · CGHS Diagnostic Centres Delhi NCR → · MRI vs CT Scan → · Fibroscan Cost Delhi →



.png)